
DISCLAIMER
The draft recommendations contained herein were preliminary drafts submitted for discussion purposes only and do not constitute final determinations. They have been subject to modification, substitution, or rejection and may not reflect the adopted positions of IFATCA. For the most current version of all official policies, including the identification of any documents that have been superseded or amended, please refer to the IFATCA Technical and Professional Manual (TPM).
57TH ANNUAL CONFERENCE, Accra, Ghana, 19-23 March 2018WP No. 161ATCOs and Colour VisionPresented by PLC |
Summary
The issues surrounding colour vision deficiency testing were examined in WP165L at the Toronto conference 2017. This follow up paper looks in more detail at the subject, and includes a more in-depth study of testing regimes across the world.
It also follows up on further work carried out by ICAO on the subject as a result of working paper WP104 presented at the 39th ICAO Assembly regarding colour vision testing.
Introduction
1.1. This paper follows on from last year’s working paper ’ATCOs and colour vision’, which contained the following recommendations;
- Further study is carried out by IFATCA outside Europe to determine the extent of colour vision testing, and the pass criteria used.
- The IFATCA EB seek clarification from EASA/ ICAO on pass criteria for colour vision testing.
Discussion
2.1. Working paper WP165L (2017) investigated the issues around colour vision deficiency testing. Appendix A contains information from that paper detailing what colour vision deficiency is, how it is tested, and the requirements for testing. The WP found the following conclusions;
2.1.1. There are a number of tests available to colour vision deficiencies; the main ones in current use being Ishihara pseudoisochromatic plates, the Nagel anomaloscope, and the Colour Assessment Display (CAD) test. At the current time the CAD test is the most effective at detecting Red/ Green (R/G) and Yellow/ Blue (Y/B) deficiencies.
2.1.2. Criteria for passing colour vision testing are described in a number of different documents and are both incomplete and contradictory.
2.1.3. ICAO annex 1 requires applicants “to demonstrate the ability to perceive readily those colours the perception of which is necessary for the safe performance of duties”. It specifies only the use of pseudoisochromatic cards, such as Ishihara. ICAO have the same colour vision requirements for both a class 1 and a class 3 medical certificate.
2.1.4. ICAO8984 which provides guidance material, acknowledges that “there is very little information which shows the real, practical implications of colour vision defects on aviation safety”. It also recognises the inconsistency between the methods and criteria used by different States. Significantly they suggest “a challenge remains to determine exactly where the cut-off between “safe” and “unsafe” should be with respect to an initial applicant who chooses aviation as his career or “hobby” .
2.1.5. EASA ED 2015/010/R Annex IV. states that applicants should be normal trichromats. The use of pseudoisochromatic cards alone is insufficient; and it suggests the use of an anomaloscope (with a matching range of 4 or less) or CAD test (with no pass mark specified).
2.1.6. Eurocontrol ‘Requirements for European Class 3 Medical Certification of Air Traffic Controllers’ specifies “normal colour perception is required”, and defines this as “the ability to pass the Ishihara test or to pass an anomaloscope as a normal trichromate”.
2.1.7. CAP1429 define three levels of colour vision capabilities; normal trichromatic vision, functionally normal trichromatic colour vision (CAD 2.35 Standard Normal units (SN) or less) and safe trichromatic colour vision (CAD 4SN or less).
2.1.8. Under ICAO regulations, pilot requirements are the same as for controllers. EASA regulations however specify “Applicants shall be required to demonstrate the ability to readily perceive the colours that are necessary for the safe exercise of the privileges of the applicable licences”. Further testing is only required if an Ishihara test is failed. Pass criteria are detailed within ANC2 MED B.075, but are different to those detailed for controllers. Unlike pilots, controllers face mandatory secondary testing and a Colour Vision (CV) requirement that is 3 times higher.
2.1.9. CAP1429 details the difficulties in setting appropriate pass criteria, given the lack of research into what would be the correct balance between ensuring safety and unfairly penalising applicants with a colour vision deficiency. The various different pass criteria suggested are reproduced in this document.
2.1.10. There is evidence to suggest that testing of colour vision at renewal of a medical certificate varies from country to country. In Canada and Italy for example, controllers are currently routinely tested using the Ishihara test (every two years for those under 40 years of age, and yearly for those above). Controllers in the UK, and Belgium have been tested previously, but this is not currently a requirement.
Colour vision deficiency testing in the UK
3.1. The original paper WP165L (2017) was written as a result of an issue raised with the UK Member Association (GATCO). A student Air Traffic Controller was denied a medical certificate on the basis of failing a CAD test for colour vision deficiency, despite no pass criteria being laid down. Discussions took place between GATCO and the UK CAA regarding the lack of detailed criteria.
3.2. Subsequent to this, in July 2017, the UK CAA issued revised policy on colour vision testing. The new policy in PART.ATCO.MED.B.075 of the EU Regulation 206/2011 states;
| In the UK, all Aeromedical Centres (AeMCs) shall use the CAD test to measure the colour thresholds for initial applicants for EU class 3 certificates.If the CAD test demonstrates thresholds for R-G for 1.79 or less with a diagnosis of normal trichromacy, the test is considered acceptable for certificate issue.
If the CAD test demonstrates thresholds of 1.79-2.35 CAD units, the result must be referred to the CAA. Additional testing may be required, but with reference to CAP 1429, thresholds between these values will normally be accepted as being of a functionally normal trichromat, i.e. there is a very mild colour deficiency but the applicant performs the same as people with normal colour vision. |
3.3. CAP 1429, Analysis of European colour vision certification requirements for air traffic control officers (2016), looked at a number subjects with colour vision loss, and derived equivalence between performance on lantern tests and the corresponding CAD threshold. This, together with analysis of evidence from conventional tests (such as Ishihara) led to statistical equivalence between historically accepted pass / fail limits and the severity of colour vision loss as measured on the CAD test. Thus, they proposed CAD threshold limits that corresponded to 100% correct performance on the HW-A lantern. They suggested that this approach provides justifiable ‘colour safe’ standards based on CAD thresholds.
3.4. The conclusions of the paper were that there were three categories of colour vision that could be used to describe trichromatic colour vision (the required standard of colour vision):
1. ‘Normal’ trichromatic Colour Vision (CV1).
2. ‘Functionally normal’ trichromate Colour Vision (CV2). This is people with CVD, Y/B thresholds within the normal range, but whose R/G CAD test result was 2.35 or less.
3. ‘Safe’ trichromatic Colour Vision (CV3). This is people with Y/B CAD thresholds within the normal range and R/G thresholds of 4 or less.
3.5. Using a CAD test pass mark of 2.35 aligns with the previously stated definition of a ‘functionally normal’ trichromate (as per 3.4. above). CAP1429 stated that; ”Based on these findings, a CV2 pass would be appropriate for air traffic controllers” (CAP1429, p.83).
3.6. However, it also suggests that “the CV3 category is appropriate for the majority of normal working environments that employ suprathreshold colours and do not involve discrimination of fine colour differences or the need to make correct judgements of colour appearance” (CAP1429, p.14). “With appropriate design and choice of colours, the CV3 category can also be appropriate for use in the ATC environment as well as in many other occupations that involve the use visual displays” (CAP1429, p.15). This suggests that in certain conditions, a higher pass mark could be applied.
ICAO and colour vision
4.1. A paper was presented at the 5th Asia Pacific Regions (RASG-APAC/5) in October 2015, by New Zealand and Australia (WP/26) concerning the lack of international harmonisation in States’ application of colour vision deficiency standards. The paper recommended that “ICAO clarifies and specifies its Colour Vision Deficiency Standards”.
4.2. As a result, A39-WP/104- ‘Lack of international harmony in the application of aviation colour vision standards’ was presented at the 39th ICAO conference in September 2016. This paper highlighted many of the issues raised in the paper on colour vision deficiency testing paper presented by GATCO at the 2017 IFATCA conference (reference), namely;
4.2.1.
“questions and uncertainties about the aeromedical significance of needing to recognise specific colours in aviation and how to best test for these”.
4.2.2.
“a high degree of variation between States in the detection and medical assessment of applicants in aviation with colour vision deficiency, and that this variation stems from the application of medical Standards rather than the wording of the Standards themselves”.
4.3. The paper made the following recommendations;
“The Assembly is invited to recommend that ICAO reviews its colour vision deficiency standards in the interests of assisting international harmonisation, including:
a) identification of the specific role colour recognition plays in the aviation environment
b) the updating of acceptable testing modalities to reflect current requirements for colour vision in aviation, and
c) a recommended application of testing results against these standards”.
4.4. The minutes from the 39th ICAO conference stated that:
“The Commission reviewed A39-WP/104, presented by New Zealand, Australia and Singapore, which recommended that ICAO specify the role of colour recognition in aviation and clarify the application of Standards for the assessment for colour vision deficiency. The Commission acknowledged the complexity of colour vision assessment and its uniform application, which would require ICAO to review the feasibility of harmonization. The Commission supported the paper and agreed that the issue should be referred to the Council for further consideration taking into account existing priorities funded through the 2017-2019 Budget and the availability of extra-budgetary resources”.
4.5. In June 2017, the Chief of the Airspace Management and Optimization Section (AMO) of the Air Navigation Bureau reported that
“ICAO is putting together a work group to review the role of colour vision in aviation and associated standards. A number of experts has been identified. Initial work will be done electronically. Start date by the end of this month”.
4.6. A further update was received from the Chief of the Aviation Medicine Section at ICAO, who stated that “I am busy with drafting of the documentation for TOR and the deliverables”, with further details due in early 2018. The author of this paper has been invited to be part of this working group. IFATCA will be advised of any pertinent updates from this group as appropriate.
Survey of worldwide colour vision testing
5.1. A survey was conducted to determine the different testing regimes and associated pass criteria. The survey was sent to all MAs and conducted using ‘survey monkey’. The questions contained within the survey are included within appendix B.
5.2. Responses were received from 30 countries, covering all of the IFATCA regions. Analysis of the results showed a large variety of testing regimes.
5.2.1. The majority (13) of respondants reported that tests were carried out using the Ishihara tests, with just three using the CAD test, one using the Beyne lantern test and two using the anomaloscope test. Of those countries using the CAD test only one (UK) was able to provide the formal pass mark recorded. Of those using the Ishihara test, both those who provided a pass mark, stated that it was 2 or less errors on a standard 24 plate test. Only two countries were required to undergo a second test despite passing the first test.
5.2.2. Despite EASA rules stating that the use of pseudoisochromatic cards alone is insufficient suggesting the use of an anomaloscope or CAD test, only two European countries out of 18 reported the use of an additional test; one using the CAD test and one anomaloscope.
5.2.3. In terms of what regulations are used, four out of five countries that responded within the Americas region used ICAO regulations, with the other using national regulations. In Europe, five out of the eight countries that responded to this question used EASA regulations, with the other three using national regulations.
5.2.4. There was a discrepancy also in testing at renewal. A majority of countries (five out of seven respondents) in the European region confirmed that Controllers were required to undergo a colour vision test at the renewal of their medical certificate, while others in the same region were not. EASA regulations do not require colour vision to be tested at medical renewal. Only three out of fourteen countries that replied, stated that testing at renewal was not required.
5.2.5. Several countries provided their national regulations. In Australia for example, the relevant document; Civil Aviation Safety regulations 1998- REG 67.160 specifies that applicants; “Can readily distinguish the colours that need to be distinguished for the safe exercise of privileges, or performance of duties, under the relevant licence”. This can be demonstrated by “in daylight, or artificial light of similar luminosity, readily identifying a series of pseudo-isochromatic plates of the Ishihara 24-plate type, making no more than 2 errors”. No further tests are specified.
5.2.6. In Canada, Part IV – Personnel Licensing and Training, Canadian Aviation Regulations (CARs) 2017-2, Standard 424 – PHYSICAL AND MENTAL REQUIREMENT 1.39, states; “The candidate shall be required to demonstrate his ability to perceive readily those colours the perception of which is necessary for the safe performance of his duties.” Various tests are listed using pseudoisochromatic plates along with pass marks: for comparison with the Australian regulations, 2 errors on a standard 24 plate Ishihara test. If an applicant does meet the standard, it continues: “the applicants colour vision shall be assessed fit under this requirement if he passes a Canadian Forces or Civil Aeronautics colour perception lantern test or a Farnsworth D-15 test”.
5.3. In summary, the survey has further demonstrated the differences in colour vision testing worldwide; in terms of tests used, the regulations applied and the requirements for testing at renewal.
Use of colour in ATC
6.1. ‘Colour vision examination- A guide for employers’ published by the Health and Safety executive (UK) describes the two types of colour coding to establish specific information an employee needs to perform a task; connotative and denotative.
6.2. With connotative colour coding, colour is the only information, and the colour and its code has to be identified correctly to ensure the task can be carried out safely. Examples include specific information such as in transport systems, e.g. railway signals, or wiring standards in the electrical industry. Denotative codes enhance information provided by other distinguishing features, such as the shape of an object or text, e.g. fire extinguishers. In this case, colour is said to be used redundantly. Colour recognition is not essential but improves performance in some tasks.
6.3. Where connotative colour coding is used, good colour recognition is important. Alternatively modifications to the workplace should be considered to utilise denotative colour coding. If this is not possible, the document states that;
“…the employer is advised to prepare a medical schedule for colour vision testing that specifies the following:
– a list of the tasks in which good colour vision is important (considering efficiency and safety);
– identification of appropriate colour vision examination methods using appropriate lighting levels and types;
– a clear definition of the degree of deficiency that is acceptable (if any);”
6.4. Because of the huge variety of different tasks and equipment, it would be difficult to identify a definitive list of colours that an ATCO may have to identify to carry out their role safely. An aerodrome controller working in a Visual Control Room (VCR) and an approach controller in a radar facility for example, would be presented with significantly different palate of colours; both connotative and denotative coded.
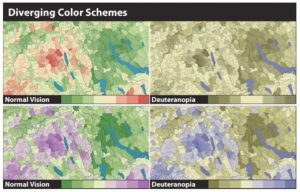
6.5. In some circumstances it is not possible to control the colours that are presented, nor the illumination levels in which they are viewed. In others however, the illumination levels can be designed to an optimum level and the colours chosen for the displays can be selected to be unambiguous to those with colour vision deficiencies. As the picture below demonstrates, changing saturation and hue can improve legibility. Additionally, reducing the amount of connotative colour coding will reduce the risk of a safety critical misidentification.
6.6. It is suggested that because of the wide range of possible scenarios as described in para 6.4 that ATCOs worldwide will work within, the use of a single colour vision test passmark may be problematic. Setting it at a level suitable for the worst case scenario would exclude those persons who could safely work in a more controlled environment. While it is accepted that having different pass marks could complicate testing regimes further, UK CAA document CAP1429 suggests that in certain conditions, a higher pass mark could be safely applied.
Conclusions
7.1. Further investigations carried out since the WP was presented in Toronto in 2017, have further highlighted the disparity between testing regimes faced by the different Member Associations within IFATCA. Even within regions covered by the same regulatory framework, differences exist in the tests undertaken/ pass criteria required to obtain an initial medical certificate, and the requirements for subsequent renewals.
7.2. The publication of a CAD test mark in the UK, based on previous research is a significant step forward. CAP1429 suggests that a higher pass mark could be safely applied.
7.3. It is accepted that it is not possible to control the colours that are presented, or illumination levels, however, use of certain colour palettes and denotative coding can improve legibility to individuals with colour vision deficiencies.
7.4. The involvement of ICAO via the Colour Vision working group, is a further encouraging development, and it is hoped that this may lead to worldwide standardisation of colour vision testing, with pass criteria specified that can be considered safe, but that do not discriminate unfairly against those with congenital colour deficiencies. IFATCA will be part of the working group, and as such will continue to monitor developments.
Recommendations
8.1. This paper is accepted as information.
References
Annex 1 to the Convention on International Civil Aviation; Personnel Licensing (2011) ICAO, Montreal
Canadian Aviation Regulations Part IV – Personnel Licensing and Training, Canadian Aviation Regulations (CARs) 2017-2, Standard 424 – PHYSICAL AND MENTAL REQUIREMENT
CAP 1429 Analysis of European colour vision certification requirements for air traffic control officers (2016)
Doc8984 (AN895)- Manual of Civil Aviation Medicine (2012), ICAO, Montreal
EASA document ED 2015/010/R Annex IV (Acceptable Means of Compliance and Guidance Material to Part ATCO.MED Medical requirements for air traffic controllers)
Requirements for European Class 3 Medical Certification of Air Traffic Controllers, Eurocontrol, Brussels
ICAO A39-WP/104 Lack of International harmony in the application of aviation colour vision standards
‘Colour vision examination- A guide for employers’ HSE available from www.hse.gov.uk/pubns/web03.pdf
Jenny, B., & Kelso, N.V., Color Design for the Color Vision Impaired in cartographic perspectives Number 57, Spring 2007
Appendix A – Background material from WP165L (2017)
1. Introduction
1.1. Within Europe applicants for ATC must obtain a Class 3 Air Traffic Controller medical certificate, which requires normal trichromatic colour vision, in order that they can correctly identify the colours of aviation lights, and effectively use the display screen equipment. Historically, Controllers were examined using tests such as the Ishihara test; recently however new tests have been introduced at initial issue of a medical certificate, and at renewa,l where the required pass standard is not clearly defined.
2. Discussion
2.1. What is colour vison deficiency and how is it tested?
2.1.1. It is generally accepted that with respect to colour perception, people fall into one of the following categories; a) Normal trichromats, who have no colour visual deficiencies (CVD). b) Deutan-like, who suffer from CVD in the green end of the red/green (R/G) spectrum. c) Protan-like, who suffer from CVD in the red end of the red/green spectrum. d) Tritan-like, who suffer from CVD in the yellow/blue (Y/B) spectrum. e) Acquired loss of colour vision.
2.1.2. There are a number of different tests currently in use to test colour vision.
2.1.2.1. Ishihara
2.1.2.2. The most commonly used method for testing colour vision at the initial issue of medical certificate is pseudoisochromatic cards, such as Ishihara Test Cards. This method uses the first 15 cards, presented in a random order, from a 24 card deck. The Ishihara Test User Manual states that a score of 13 or more correct indicates normal colour vision, and this criteria was used prior to 2009. Since then the pass criteria has been changed to zero errors. It only tests for R/G CVD, and is able to distinguish if a subject is Deutan-like or Protan-like, but without any measure of severity.
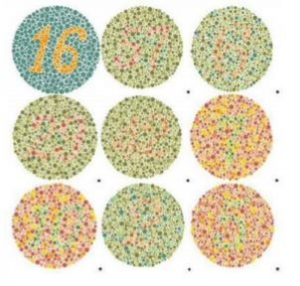
2.1.2.3. It has however been shown that the Ishihara test can produce false negatives for normal trichromats, who would subsequently be failed. To overcome this issue of ‘failed’ normal trichromats, a second test, such as a lantern test or an anomaloscope test was introduced. These methods have almost 100% success rate in picking up false negatives in normal trichromats. However, neither of these methods will pick up Y/B CVD.
2.1.3. CAD test
2.1.3.1. The CAD test was developed by City University, London, and:
“is implemented on a calibrated visual display and consists of coloured stimuli of precise chromaticity and saturation that are presented moving along each of the diagonal directions of a square foreground region made up of dynamic luminance contrast noise. The subject’s task is to report the direction of motion of the colour-defined stimulus by pressing one of four appropriate buttons” (CAP1429, p.39).

2.1.11. Nagel anomaloscope
2.1.11.1. The Nagel anomaloscope is based on colour matching; it has a disc that consists of two half fields and is viewed in an optical system. The top half is illuminated by a mixture of spectrally narrow red and green wavelengths; the lower half by spectrally narrow yellow light. Two control knobs are used, one to alter the red-green colour mixture ratio in the top field, and one to alter the luminance of the lower field. The subject is then required to match the two halves of the circle completely in both colour and brightness by using the control knobs. The second part of the test is to determine the limits of matching range.
2.1.11.2.
“Normal Nagel match parameters have however been recorded in a small number of subjects with clear loss of RG sensitivity as assessed using the CAD test. Similarly, a large variation in match midpoint in ‘normal’ trichromats have been noted in other studies” (CAP1429, P.36).
2.2 Requirements to obtain an ATCO medical certificate
2.2.1 ICAO annex 1, chapter 6; Medical provisions for licensing sets out the requirements for medical certification. It states that commercial and air transport pilots are required to undergo a class 1 medical assesment, and Air traffic controllers a class 3 medical assesment. There is no differential between the assesment required for an ICAO class 1 or a class 3 certificate. The requirements state;
2.2.1.1
| 6.2.4 Colour perception requirements6.2.4.1 Contracting States shall use such methods of examination as will guarantee reliable testing of colour perception.
6.2.4.2 The applicant shall be required to demonstrate the ability to perceive readily those colours the perception of which is necessary for the safe performance of duties. 6.2.4.3 The applicant shall be tested for the ability to correctly identify a series of pseudoisochromatic plates in daylight or in artificial light of the same colour temperature such as that provided by CIE standard illuminants C or D65 as specified by the International Commission on Illumination (CIE). 6.2.4.4 An applicant obtaining a satisfactory result as prescribed by the Licensing Authority shall be assessed as fit. An applicant failing to obtain a satisfactory result in such a test shall be assessed as unfit unless able to readily distinguish the colours used in air navigation and correctly identify aviation coloured lights. Applicants who fail to meet these criteria shall be assessed as unfit except for Class 2 assessment with the following restriction: valid daytime only. |
2.2.1.2 However 11.8.34 warns that;
“A problem with colour plates is that they detect very mild colour vision defects which might not be significant in the aviation environment. In other words, they are rather too discriminating”.
2.2.1.3 ICAO document 8984 Manual of Civil Aviation Medicine (2012) provides guidance on suitable methods for assessing colour vision as described above. It states;
2.2.1.4
| 11.8.10 The applicant shall be required to demonstrate ability to perceive readily those colours the perception of which is necessary for the safe performance of his duties. Precise physical and physiological criteria cannot be given because of the large number of variables in different viewing situations. |
2.2.1.5
| 11.8.29 The problem with colour vision standards for pilots and air traffic controllers is that there is very little information which shows the real, practical implications of colour vision defects on aviation safety. Ideally one would select only applicants with normal colour vision as measured by the most discriminating tests. This policy would deny licences to a significant number of individuals who might be able to function safely in the aviation environment. The question is where to draw the line. Many Contracting States simply define as acceptable those applicants who obtain a certain score with an authorized set of pseudo-isochromatic test plates, others accept as “colour safe” colour-deficient applicants who pass certain additional tests. |
2.2.1.6
| 11.8.40 Some States use the term “colour vision defective safe” or “colour safe” to refer to individuals who fail the colour plate tests but can pass testing with an anomaloscope or an accepted colour lantern test or both, and the term “colour vision defective unsafe” or “colour unsafe” to refer to those individuals who fail both plates and anomaloscopy and lantern tests. Despite all the work undertaken concerning colour vision, a challenge remains to determine exactly where the cut-off between “safe” and “unsafe” should be with respect to an initial applicant who chooses aviation as his career or hobby. |
2.2.1.7
| 11.8.43 There is no internationally agreed, standardized method for evaluating colour vision in persons working in the aviation environment. Some Contracting States test all flight crew and air traffic controllers on a regular basis and test each eye separately using a method which screens for yellow-blue defects in addition to the more common red-green defects. This allows detection of the uncommon but important acquired colour vision defects”. |
2.2.1.8 ICAO document 8984 Manual of Civil Aviation Medicine (2012) has the same broad colour vision requirements for a class 1 and class 3 medical certificate, but does not have specific pass figures.
2.2.2 European medical certification requirements (EMCR) were originally contained in the Eurocontrol document ‘Requirements for European Class 3 Medical Certification of Air Traffic Controllers’. While they are still referenced by the websites of a number of states, they have been superceded by the EASA document described below.
2.2.2.1 EMCR 15.1(a) states;
| “Normal colour perception is required. It is defined as the ability to pass the Ishihara test or to pass an anomaloscope as a normal trichromate. 15.1.1 The Ishihara test is to be considered passed if consecutive plates are identified correctly as specified in the Ishihara User Manual.
15.1.2 Those failing the Ishihara test shall be examined by: anomaloscopy (Nagel or equivalent). This test is considered passed if the colour match is normal trichromatic. 15.1(b) An applicant who fails the acceptable colour perception tests is to be considered colour unsafe and shall be assessed as unfit. |
2.2.3 When it comes to colour vision testing, EASA have different requirements for Class 3 (ATCO) and Class 1 (pilot) medical certificates. The relevent document for EASA is ED 2015/010/R Annex IV (Acceptable Means of Compliance (AMC) and Guidance Material (GM) to Part ATCO.MED Medical requirements for air traffic controllers). Both AMC and GM are nonbinding.
2.2.3.1 For a class 3 medical it requires that “applicants shall be normal trichromats”.
2.2.3.2 AMC 1 ATCO MED B 075 (colour vision) states;
| (a) Pseudoisochromatic plate testing alone is not sufficient (b) Colour vision should be assessed using means to demonstrate normal trichromacy. (p. 33) |
2.2.3.3 GM 1 ATCO MED B 075 states;
| The means to demonstrate normal trichromacy include: (a) anomaloscopy (Nagel or equivalent). This test is considered passed if the colour match is trichromatic and the matching range is four scale units or less;
(b) Colour Assessment and Diagnosis (CAD) test. |
2.2.4 CAP 1429, Analysis of European colour vision certification requirements for air traffic control officers (2016), was produced by the CAA, in collaboration with City University, London, where the CAD test was developed.
2.2.4.1 This study looked at a number subjects with colour vision loss, and derived equivalence between performance on lantern tests and the corresponding CAD threshold. This, together with analysis of evidence from conventional tests (such as Ishihara) led to statistical equivalence between historically accepted pass / fail limits and the severity of colour vision loss as measured on the CAD test. Thus, CAD threshold limits were proposed that corresponded to 100% correct performance on the HW-A lantern. They suggest that this approach provides justifiable ‘colour safe’ standards based on CAD thresholds.
2.2.4.2 The conclusions of the paper were that there were three categories of colour vision that could be used to describe trichromatic colour vision (the required standard of colour vision):
| 1. Normal’ trichromatic Colour Vision (CV1). 2. Functionally normal’ trichromate Colour Vision (CV2). This is people with CVD, Y/B thresholds within the normal range, but whose R/G CAD test result was 2.35 or less.
3. ‘Safe’ trichromatic Colour Vision (CV3). This is people with Y/B CAD thresholds within the normal range and R/G thresholds of 4 or less. |
2.6 Renewal of a medical certificate
2.6.1 There is currently no requirement for colour vision to be tested for when a class 3 medical certificate is renewed. However ICAO8984 11.8.41 describes several acquired colour vision defects.
2.6.2
| “Although much less common than congenital defects, acquired colour vision defects do occur. These may affect one eye more than the other and may be progressive. The more important causes include: a) Tapeto-retinal degenerations and pigmentary retinopathies;
b) Chorioretinitis from any cause including macular lesions; c) Optic neuropathy from any cause including advanced glaucoma; d) Drug toxicity affecting the macula or the optic nerve”. |
2.6.3 CAP1429 recognises this need for subsequent testing; “Since changes in chromatic sensitivity are often indicative of early-stage systemic (e.g. diabetes) or ocular diseases (e.g. glaucoma, age-related macular degeneration), it may be appropriate for both RG and YB colour sensitivity to be assessed regularly at medical examinations” (CAP1429, p.27).
2.6.4 Since CAD is very good at detecting progressive Y/B deficiencies, it is a useful tool to use to detect early onset of age or condition related CVD that may require further investigation. This makes it a better tool to use for medical renewals, as well as initial assessments, as it is as quick as a Ishihara Test, but has the added benefits of detecting Y/B issues, which Ishihara does not.
2.6.5 EASA regulations for a class 1 (pilot) medical states; “at revalidation and renewal examinations, colour vision shall be tested on clinical indication”. Significantly, it states; “this test (CAD) is considered passed if the threshold is less than 6 standard normal (SN) units for deutan deficiency, or less than 12 SN units for protan deficiency. A threshold greater than 2 SN units for tritan deficiency indicates an acquired cause which should be investigated”. (SN is a Standard Normal (CAD) unit, and is a measure used to describe varying levels of luminance contrast).
2.6.6 The Belgian Guild of Air traffic controllers reported that a test of colour vision was introduced at medical renewal, and some controllers were diagnosed with colour blindness (which had not been a problem at their previous medical examinations) and therefore would not be able to exercise the privileges of their license. After negotiations, it was decided they had to undergo more accurate testing concerning the colours actually used on their CWPs instead of the ones tested by the Ishara method.
2.6.7 When UK licences changed from class 1 to class 3 in 2009, the document European class 3 medical certification of air traffic controllers: UK CAA guidance stated;
“there may be exisiting UK class 1 certificate holders, who have a particular medical condition that has been deemed acceptable under the UK class 1 medical requirements before 1st September 2009, that do not meet the new European class 3 medical requirements.If the AMS is satisfied that the controller is able to exercise the priviledges of the license, UK class 1 medical requirements may continue to apply in respect of the specific medical condition only . The AMS will impose a grandfather rights limitation (IGR) accordingly on the European class 3 medical certificate. In all other respects and for any new medical condition the controller may develop on or after 1st September 2009, the European class 3 medical requirements will apply”.
2.6.8 A requirement to undergo colour vision testing at medical renewal was introduced briefly in the UK in 2013. The UK controllers association GATCO, described the case of one now retired controller who failed both an Ishihara and CAD test (he had failed an Ishihara test at initial medical examination but passed a lantern test and was deemed fit to work. Despite scoring higher on the CAD than any pilot or controller scores detailed above, it was decided that as he had worked for around 30 years without problems as both a tower and centre controller, that grandfather rights should apply and he was allowed to continue to exercise the privileges of his license.
2.6.9 It is estimated that potentially as much as 2%, or 1 in 50 of people could fail if they introduced colour vison testing at renewal using the CAD test at the level used in the UK.
Appendix B – Survey Questions
Q1. In which country do you work?
Q2. On initial medical testing, what tests are carried out for colour vision? (tick all that apply) Ishihara, CAD, Anomalascope, Other (please specify)
Q3. If more than one test is used, is that only if the first test is failed?
Q4. Under what regulations is colour vision testing carried out? (eg EASA/ ICAO/ National regulations?)
Q5. What pass mark is used for the CAD test (if used)?
Q6. Is the CAD test pass mark specified in writing anywhere?
Q7. Is colour vision tested at medical renewal?
Q8. If colour vision is tested at renewal, what method is used? (tick all that apply) Ishihara, CAD, Anomalascope, Other (please specify)
Q9. Is the pass criteria the same for intial testing and renewal?
Q10. If the pass criteria is different at renewal, what is it?

