
50TH ANNUAL CONFERENCE, Amman, Jordan, 11-15 April 2011WP No. 94Study Hypoxia WarningPresented by PLC and TOC |
Summary
Hypoxia is a condition in which the body is deprived of sufficient oxygen. Several accidents and near- accidents have happened in aviation in the past due to hypoxia. This study provides information on the phenomenon and includes guidelines for ATCOs when encountering pilots with hypoxia.
This working paper provides information material and is recommending to amend IFATCA Policy on the issue.
Introduction
1.1 The IFATCA Technical and Operations Committee and the Professional and Legal Committee were tasked to investigate the phenomenon of hypoxia.
1.2. Hypoxia is a pathological condition in which the body as a whole or a region of the body is deprived of adequate oxygen supply. A mismatch between oxygen supply and its demand at the cellular level may result in a hypoxic condition.
1.3. Hypoxia in aviation can only occur to aircrew and passengers; nevertheless, it could be a benefit if ATCOs were informed about the phenomenon of hypoxia when encountering abnormal changes in pilot behaviour.
1.4 The ability to recognize / detect personal impairments was discussed at the IFATCA Conference in Punta Cana in WP No. 159 “Detecting impaired personal performance”. The ability to detect impaired performance in other people is the most important aspect of the process.
Discussion
2.1 When a human body fails to acquire sufficient oxygen, the body will get into a condition, which is called hypoxia or “altitude sickness.” This condition can have a gradual or rapid onset. A rapid onset of hypoxia could occur when aircraft oxygen-supply systems at higher altitudes (above FL140) fail to supply the correct amount or correct composition of oxygen. An example of gradual onset would be prolonged cruise just above 10000 feet above MSL.
2.2. ICAO References
ICAO has publications on hypoxia in Doc 8984 Manual of Civil Aviation Medicine:
Hypoxia in simple terms is a lack of sufficient oxygen to keep the brain and other body tissues functioning properly. Wide individual variation occurs with respect to susceptibility to hypoxia. In addition to a progressive lack of oxygen at higher altitudes, anything interfering with the blood’s ability to carry oxygen can contribute to hypoxia (anaemias, carbon monoxide, tobacco and certain drugs). Also, alcohol and various drugs decrease the brain’s tolerance to hypoxia. Your brain has no built-in alarm system to let you know when you are not getting enough oxygen. It is impossible to predict when or where hypoxia will occur during a given flight, or how it will manifest itself. A major early symptom of hypoxia is an increased sense of well-being (referred to as euphoria). This progresses to slowed reaction, impaired thinking ability, unusual fatigue, and a dull headache feeling. The symptoms are slow but progressive, insidious in onset, and are most marked at altitudes starting above 10 000 feet. Night vision, however, can be impaired starting at altitudes lower than 10 000 feet. Smokers may also experience symptoms of hypoxia at lower altitudes than non-smokers If you observe the general rule of not flying above 10 000 feet without supplemental oxygen, you will not get into trouble.
2.3 IFATCA
2.3.1 IFATCA has no policy on hypoxia.
2.3.2 IFATCA Policy on Emergency Training [TRNG 2.8]:
| Emergency training, including Flight Emergency Response (IFER) and Coordination training, handling of Unlawful Interference situations should be part of ab-initio and refresher training. |
If IFATCA were to accept policy on hypoxia, this could be an excellent place to insert the policy. If applicable, examples of relevant accidents and accidents could provide more clarity in addition to theoretical emergency training.
2.4 International Federation of Airline Pilots Associations (IFALPA)
IFALPA policy on hypoxia is:
Initial and periodic recurrent training should include hypoxia awareness and examples of relevant accidents. This training could be incorporated into the Crew Resource Management or other refresher training.
2.5 Signs and symptoms
2.5.1 The symptoms of generalized hypoxia depend on its severity and acceleration of onset. In the case of altitude sickness, where hypoxia develops gradually, the symptoms include headaches, fatigue, shortness of breath, a feeling of euphoria and nausea. In severe hypoxia, or hypoxia of very rapid onset, changes in levels of consciousness, seizures, coma, and death occur. None of these symptoms are conducive to safe operation of aircraft and must be recognized in time for effective treatment.
2.6 Medical background
2.6.1 “The percentage of oxygen in air, at 21%, remains almost unchanged up to 7,000 feet (2,100 m). Consequently, the available amount of oxygen to sustain mental and physical alertness decreases above 10,000 feet (3,000 m). Although the cabin altitude in modern passenger aircraft is kept to 8,000 feet (2,400 m) or lower, some passengers on long-haul flights may experience some symptoms of altitude sickness.”
Hypoxia’s causes can be classified as:
- Hypoxemic hypoxia – a low partial pressure of oxygen in arterial blood that may be due to low partial pressure of atmospheric; inadequate pulmonary ventilation (e.g., in chronic obstructive pulmonary disease or respiratory arrest); or shunts in the pulmonary system.
- Hypemic hypoxia in which arterial oxygen pressure is normal, but total oxygen content of the blood is reduced due to carbon monoxide poisoning; which inhibits the ability of hemoglobin to release the oxygen bound to it.
- Histotoxic hypoxia in which quantity of oxygen reaching the cells is normal, but the cells are unable to effectively use the oxygen due to disabled oxidative phosphorylation enzymes.
- Ischemic, or stagnant hypoxia in which there is a local restriction.
Adequate oxygen saturation of hemoglobin is vital to human function. Above 10,000 feet, the amount of hemoglobin in the blood begins to decrease much more rapidly, much faster than air pressure, which continues to decrease at a similar rate. By 20,000 feet altitude, the concentration of hemoglobin in the blood is only 65% saturation and at these levels, normal human function is materially interrupted and the effects are cumulative over time. At higher altitudes, the effects worsen quickly.
2.7 Technical background
2.7.1 Aircraft Pressurization System
Aircraft, which routinely operate above 10,000 feet altitude, are pressurized to keep the aircraft cabin no higher than the equivalent of 8000 feet altitude at any actual altitude up to the prescribed maximum operating altitude. The partial pressure of oxygen is equivalent to the prevailing “Cabin Altitude”. The existence of an air pressure inside the aircraft pressure hull, which is never less than that outside it, implies the existence of a pressure differential between outside and inside the aircraft. Aircraft pressurization systems normally operate automatically and monitoring correct operation by reference to cabin altitude, cabin rate of climb and descent, and differential pressure is the only routine requirement.
2.7.2 Aircraft Supplementary Oxygen Systems
Aircraft that are certificated to operate above 10000’ MSL in daytime or 8000’ at night are required to carry supplemental oxygen for all occupants. The pilots usually have a fixed oxygen system consisting of an oxygen source, regulator, and mask. Passengers are provided with a similar capability but in modern aircraft the oxygen source is a chemical generator providing oxygen above 14000’MSL for duration of around 15 minutes or less. Occupants with a known medical condition may carry oxygen onboard or have a generator/condenser. Requirements for the carriage and use these systems are spelled out in regulation and the aircraft operations manual.
2.7.3 Automatic Emergency Descent Mode
Some autopilot systems have an automatic emergency descent mode. If, when flying above e.g. 30,000 feet, the cabin depressurizes, the autopilot will automatically start an emergency descent at maximum speed. Some systems require the pilots to retard the power and extend the speedbrakes for maximum descent rate, but the autopilot will automatically maximize the descent rate until it captures and holds 15,000 feet awaiting further pilot input.
2.8 Risk scenarios
2.8.1 The possibility of hypoxia from technical failures arises in two very different ways:
- Sudden loss of normal cabin pressurization at high altitude due to a rapid or explosive decompression (RD) resulting from a structural failure or aircraft system failure.
- Gradual and progressive onset during flight above 10,000 feet altitude in the absence of normal pressurization. This can arise by climb above 10,000 feet without either the pressurization system functioning, or because it is functioning incorrectly due to malfunctioning or incorrect settings.
2.8.2 A more insidious form arises from a medical condition known or unknown to the pilot that affects their oxygen requirements but would result in hypoxia under certain conditions.
2.9 Time of useful consciousness
2.9.1 The Time of Useful Consciousness (TUC) or Effective Performance Time is the period of elapsed time from the interruption of normal air supply or exposure to an oxygen-poor environment until the time when the ability to functional usefully is likely to be lost at which point an affected individual would no longer be capable of taking normal corrective or protective action.
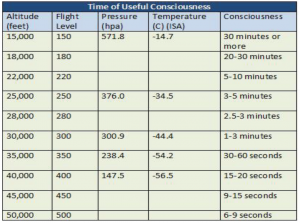
2.9.2 In the event of a rapid depressurization due to a failure of the aircraft pressurization system the TUC is decreased by one half. For example an aircraft at FL400 with a rapid depressurization has a TUC of 7 to 10 seconds before coherent behaviour is lost, which is normally 15 to 20 with a gradual depressurization.
2.10 Relevant accidents and incidents
2.10.1 For recent aircraft decompression accidents at altitude refer to:
- 1999 South Dakota Learjet crash (the crash which claimed the life of golfer Payne Stewart)
- 2000 Australia Beechcraft King Air crash
- Helios Flight 522
- Soyuz 11 fatal spacecraft decompression on re-entry
2.10.2 On 14 August 2005 a B737 belonging to Helios Airways crashed following the incapacitation of the crew due to hypoxia. According to the official report into the accident published by the Hellenic republic Ministry of Transport & Communications:
“The direct causes were:
- Non-recognition that the cabin pressurization mode selector was in the MAN (manual) position during the performance of the Preflight procedure, the Before Start checklist and the After Takeoff checklist.
- Non-identification of the warnings and the reasons for the activation of the warnings (Cabin Altitude Warning Horn, Passenger Oxygen Masks Deployment indication, Master Caution).
- Incapacitation of the flight crew due to hypoxia, resulting in the continuation of the flight via the flight management computer and the autopilot, depletion of the fuel and engine flameout, and the impact of the aircraft with the ground.”
2.10.3 On July 26 2008 in a Learjet of Kalitta Charters, working with Cleveland Center and flying to Ypsilanti Michigan, the flight crew encountered hypoxia. What followed was a bizarre radio communication between the controllers and the pilots, even involving inputs from pilots from other flights. It took the controllers a considerable amount of time to realize that hypoxia was the reason for the strange behaviour of the intoxicated pilots. When the reason for the behaviour was clear to the controllers, the situation was soon under control when the controller issued a descent clearance to the flight to regain sufficient oxygen. The pilots were unaware of their own behaviour and intoxication, and without the controller input it may not have been possible to resolve this situation.
2.10.4 Previously mentioned accidents and incidents clearly show the need for awareness of hypoxia among ATCOs. Incidents like with Kalitta 66 could easily escalate into complex and dangerous situations influencing numerous flights in the same (high density traffic) airspace. Therefore TOC and PLC consider it necessary for ATCOs to be aware of the effects of the hypoxia phenomenon, and therefore this should be included in ATCO training.
2.11 Training
2.11.1 Pilot Training Programs
Pilot training generally does address hypoxia. For example, pressure chambers are used in aviation to highlight the pilot’s awareness of physiological and cognitive impairments. In such experiments the aircrew is asked to carry tasks such as writing, reading and operating devices while the pressure is gradually decreasing. The purpose of these experiments is to allow aircrew to feel the pressure decrease by the impairments in performance when carrying out their tasks. By being aware of the physiological and cognitive impairment when pressure decreases, the assumption is that the individual could be more aware and thereby able to identify hypoxia and alert him/herself and the other crewmembers of a potential or active urgency. Once facing this situation the aircrew member could develop a personal alert /red traffic light or detect impairments among the other crewmembers. Usually only military pilots receive this kind of training.
2.11.2 PLC Working Paper 159 (IFATCA Conference 2010) “Detecting impaired personal performance”, paragraph 2.8.4 mentions:
“As with many simple and effective models, attempts have been made to add to the conscious competence model, notably a fifth stage normally represented as: ‘Conscious competence of unconscious competence’, which describes a person’s ability to recognize and develop unconscious incompetence in other.”
The first step in this learning process is being aware of impaired performance like hypoxia, and the easiest way to achieve awareness is by discussing the problem openly. Furthermore information should be provided on the symptoms of hypoxia and possibly include in an ATCO emergency- checklist
As mentioned in the conclusion of WP 159 (IFATCA Conference 2010), Team Resource Management (TRM) should be extended to make ATCOs and other team workers aware of detecting signs of impaired performance of their colleagues. Hypoxia is an excellent example of how we can detect signs of impaired performance of colleagues, in this case not our ATC colleagues, but the pilots that are incapacitated due to hypoxia.
2.11.3 ICAO Guidance on ATCO Procedures
It is very difficult for ATCOs to identify the phenomenon of hypoxia with pilots. There are no ICAO guidelines for ATCOs how to act when hypoxia occurs.
2.11.4 ATCO Training on Hypoxia Recognition and Reaction
The most probable signs for ATCOs to identify hypoxia will be strange and inconsistent behaviour by pilots, similar to an intoxicated person. In addition, illogical, incoherent, or otherwise incorrect use of radiotelephony or an uncommon way of speech could indicate hypoxia. When these signs occur, one could try to gather more information by asking questions to the pilots. However depending on the altitude of the aircraft and the severity of the loss of oxygen, the reaction time could be very limited. The key to reversing the hypoxia is recognition, getting the pilots on oxygen, and clearing the surrounding airspace. Time is of the essence. Once recognized, the solution would be to advise the pilot to put on their oxygen masks if equipped. Another way is to get the aircraft below 10.000’ MSL as rapidly as possible. Once oxygen is restored to the pilot and they are reacting normally then follow the ATCO’s SOP for reporting and analyzing the incident.
2.12 TOC and PLC consider it wise to provide ATCOs with information on the phenomenon of hypoxia. Furthermore, ATCOs should be aware of general reactions and symptoms to be able to recognize hypoxia. This should be covered during ab-initio and refresher ATCO training.
Conclusions
3.1 Hypoxia in aviation strictly affects aircrew and passengers physically, and it can lead to the incapacitation of the aircrew, which are subsequently incapable of operating the aircraft in a safe manner. Long-term exposure to hypoxia has resulted in fatalities and aircraft loss. Furthermore hypoxia, when encountered by pilots, will affect ATC operations and may jeopardize other flights in the same airspace
3.2 It is almost impossible to establish the exact reason if pilots behave strangely or abnormally. Therefore it is hard to develop standard guidelines for use by ATCOs in such a situation, however this should raise suspicion of an abnormal situation. This behavior could be linked to numerous causal factors and not only be caused by hypoxia.
3.3 TOC and PLC consider the presently available ICAO information insufficient and support IFALPA’s policy to include hypoxia in training programs for pilots. A similar course should be adopted for ATCO training, which should include hypoxia awareness and examples of associated accidents and incidents.
3.4 In some instances of a hypoxia event, which could easily result in an emergency situation, the controller may be the decisive influence in the successful outcome. Therefore IFATCA Policy on hypoxia awareness should best be added on in part TRNG 2.8 Emergency Training in the IFATCA Technical and Professional Manual.
Recommendations
It is recommended that;
4.1 IFATCA Policy, on page 4327 of the IFATCA Technical and Professional Manual:
Emergency training, including Flight Emergency Response (IFER) and Coordination training, handling of Unlawful Interference situations should be part of ab- initio and refresher training.
is amended to read:
Emergency training, including In Flight Emergency Response (IFER) and coordination training, handling of Unlawful Interference situations and Hypoxia awareness should be part of ab-initio and refresher training.
References
ICAO Doc 8984 Manual of Civil Aviation Medicine.
Skybrary: https://www.skybrary.aero/index.php/Hypoxia
Official report Helios 522 accident, Hellenic Rep. Ministry of Transport & Communications.
https://en.wikipedia.org/wiki/Hypoxia_(medical)
https://en.wikipedia.org/wiki/Altitude_sickness#Oxygen_enrichment
https://en.wikipedia.org/wiki/1999_South_Dakota_Learjet_crash
https://en.wikipedia.org/wiki/Helios_Flight_522
Kalitta66 with hypoxia: https://www.youtube.com/watch?v=_IqWal_EmBg

