
DISCLAIMER
The draft recommendations contained herein were preliminary drafts submitted for discussion purposes only and do not constitute final determinations. They have been subject to modification, substitution, or rejection and may not reflect the adopted positions of IFATCA. For the most current version of all official policies, including the identification of any documents that have been superseded or amended, please refer to the IFATCA Technical and Professional Manual (TPM).
65TH ANNUAL CONFERENCE, Bucharest, Romania, 20-24 April 2026
WP No. 159
Misuse of Psychoactive, Illicit and Controlled Substances in Air Traffic Control
Presented by PLC
| SUMMARY With the increasing legalisation of cannabis and changing social attitudes, there is an ongoing debate about positive drug tests, even when the psychoactive effects have worn off. The wider availability of cannabinoid products further fuels this discussion. The misuse of controlled substances, prescription and over-the-counter medications also presents a challenge, as some common drugs are prohibited for ATC license holders, complicating drug testing policies. The text emphasises the need for comprehensive alcohol and other drug management and education programs developed by ANSPs in collaboration with regulatory authorities and professional associations, to inform ATCOs about the regulations they must follow. |
Introduction
1.1. The World Health Organisation (WHO) defines psychoactive drugs as substances that affect mental processes like perception, consciousness, cognition or mood and emotions. Common psychoactive substances include:
— Alcohol
— Cannabis and Cannabinoid products
— Illicit drugs and
— Controlled substances and prescribed or over the counter medications
1.2. The term Illicit drugs refers to substances that are manufactured, sold or obtained illegally. Conversely controlled substances as defined by Australian Office of Drug Control (ODC) refer to a drug or chemical whose manufacture, possession, or use is regulated by a government. Misuse of controlled substances such as prescribed medications or other pharmaceuticals can make them illicit drugs.
1.3. ICAO Annex 1 – Personnel Licensing – explicitly prohibits licensed aviation personnel from operating under the influence of psychoactive substances.
1.2.7.1
Holders of licences provided for in this Annex shall not exercise the privileges of their licences and related rating while under the influence of any psychoactive substance which might render them unable to safely and properly exercise these privileges.
1.2.7.2
Holders of licences provided for in this annex shall not engage in any problematic use of substances.
1.4. Additionally, ICAO Doc 8984 (Manual of Civil Aviation Medicine) highlights the use of psychoactive substances can lead to “abuse” and dependency, often resulting in significant social, medical, legal and vocational difficulties.
1.5. According to the UK Civil Aviation Authority (CAA 2021), substance use can significantly impair the performance of licence holders. These impairments included poor judgment and decision-making skills, increased error rates and risk taking behaviour, mood changes, poor coordination, reduced tracking and concentration and slower reaction times.
1.6. In alignment with these concerns, a briefing leaflet released by the International Federation of Air Line Pilots’ Associations (IFALPA) strongly advises pilots to abstain from cannabis use. Regardless of its legal status, cannabis is deemed incompatible with flying due to its adverse impacts on cognitive, mental and physical performance.
Discussion
2.1. Impairment vs Under the Influence
2.1.1. The main area of debate is the concept of Impairment vs Under the Influence. These terms are often incorrectly used interchangeably.
2.1.2. Impairment as defined by Mirriam-Webster.com as the state of condition of being impaired: diminishment or loss of function or ability. With respect to substances it refers to a reduced or altered physical or cognitive ability.
2.1.3. Whereas, Under the Influence when used as a legal term is often defined as a breach of policy defined by a company when an employee works impaired or exhibits signs of substance abuse. A positive test result does not necessarily prove impairment but rather a violation of a company’s policy.
2.1.4. Importantly, individuals may test positive for a psychoactive substance long after its effects have worn off, yet still constitute a violation of “under the influence” policies. The debate revolves around if “under the influence” refers to active impairment (being intoxicated) or to have a detectable trace of a prohibited substance that breaches a defined policy threshold even if no observable impairment exists.
2.2. Alcohol and Cannabis: Social Norms and Testing Implications
2.2.1. The legality of psychoactive substances (particularly cannabis) varies widely across the globe, often determined by local customs, social norms and accessibility. In some countries, social use is considered acceptable, while in others it is a serious crime and punishments are as severe as the death penalty.
2.2.2. Alcohol, a psychoactive substance, is a widely accepted part of some cultures. Most people are aware of its effects, including how long it takes for those effects to wear off and be cleared from the body. This enables people to make informed decisions about when it is safe to drive, return to work, or be able to undergo alcohol screening with the expectation of a negative result.
2.2.3. Cannabis, like alcohol, is increasingly following a similar trajectory of growing social acceptance for both recreational and medicinal use, with more States moving toward legalisation. However, unlike alcohol, whose effects and metabolic rates are mostly understood, residual traces of Tetrahydrocannabinol (THC), a component of cannabis, can remain detectable in the body for an extended period long after its impairing effects have worn off. This is because the THC metabolite (THC-COOJ) is stored in fat cells and is gradually released into the blood stream over time resulting with a long elimination half life relative to other recreational drugs. (National Library of Medicine)
2.2.4. It is important to understand the difference between testing for under the influence and testing for being impaired. Currently there is no testing mechanism to be able to differentiate between them.
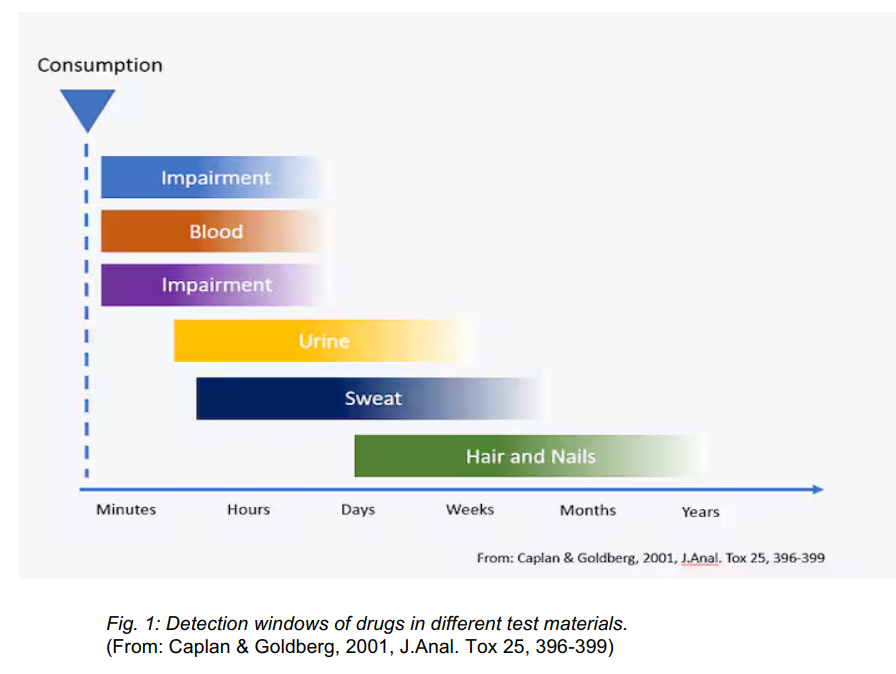
2.2.5. THC is a highly detectable substance. The detection window or “look back” period can vary from days to months depending on a variety of factors, such as the product used, the individual’s metabolism and the testing method employed.
2.2.6. In 2019 Transport Canada introduced a Cannabis 28 Day policy. Licence holders, including ATCOs, are prohibited from the use of cannabis for at least 28 days before being on duty. According to Transport Canada, 28 days was determined using the “best available science” and is consistent with other Canadian government departments’ approach to cannabis legalisation including their Department of National Defence and the Royal Canadian Mounted Police. This includes how the body gets rid of cannabis, how long it can be detected in the body and when the brain returns to normal after using cannabis.
2.3. THC vs CBD vs Hemp
2.3.1. THC is the psychoactive compound found in Cannabis which is responsible for cognitive impairment often associated with its use as a recreational drug. Cannabidiol CBD is another cannabis derivative but does not produce the same psychoactive effects typically associated with THC. CBD is often used in oils, lotions and ingestibles and often used for medicinal purposes. Hemp derived CBD products are often used in therapeutic applications. It may be used by massage therapists, chiropractors, and other practitioners and may contain trace amounts of THC. License holders may unknowingly absorb these traces through topical application or environmental exposure, possibly leading to a positive drug test result.
2.3.2. Passive exposure, such as second-hand smoke, also presents a risk—particularly in enclosed or poorly ventilated environments. While the likelihood of testing positive from passive exposure is generally low, it remains a consideration.
2.4. Drug and Alcohol Management Programs
2.4.1. MED 8.2.6 Substance Abuse in Air Traffic Control states that A programme of education of substance abuse should be made available to air traffic controllers by their employer in consultation with the MA.
2.4.2. ANSPs in conjunction with the relevant regulatory bodies and professional associations should have clearly visible and accessible drug and alcohol education programmes, policies and regulations. These initiatives are employed to ensure that substance use does not compromise the safe and effective provision of Air Traffic Control (ATC) services. These programmes aim to educate ATCOS on the dangers and consequences of alcohol and psychoactive substance use and abuse. Highlighting that substance use can compromise the cognitive ability of an ATCO to make safety critical decisions. ANSPs should regularly revisit these education programmes and the relevant policies to ensure they remain relevant and up to date.
2.4.3. To effectively manage substance related risks, these programmes typically include:
- Robust drug and alcohol policies
- Detection procedures and Testing regimes
- Worker education programmes that include
- Awareness of relevant legislation and regulations
- Up to date knowledge of emerging substances and trends.
2.4.4. In addition, self referral pathways should be available for staff who are concerned about drug and alcohol dependency. These may be facilitated through established peer support networks or other appropriate agencies, ensuring access to confidential and professional assistance. Access to these programmes should also be discrete and non punitive.
2.4.5. MED 8.2.6 Substance Abuse in Air Traffic Control states that
IFATCA Policy is:
A programme of rehabilitation from substance abuse should be made available to an air traffic controller where a problem is recognised. This programme should be set up and conducted in consultation with the MA in order to maintain the confidence and preserve the employment in ATC of the individual concerned.
2.5. Testing and detection
2.5.1. Detection of substance use is conducted through testing programmes established by regulatory authorities and/or ANSPs, and may occur in some or all of the following circumstances:
— Pre employment screening
— Random testing
— Post Incident Investigations
— Reasonable Suspicion
— Return to Duty or Follow-Up Testing
— Self-testing before the start of a duty
2.5.2. A duty of care must be placed on the appropriate authority when conducting drug tests in the workplace. These should be undertaken prior to staff members commencing shift to potentially account for the worst case scenario of a non negative test result. Random testing should also preclude gender quotas as the number of females only equate to approximately 20% of the workforce (SESAR – 2024). In some of the smaller units this ratio is less. Ensuring that female quotas are met is forcing the same individuals to be tested continuously.
2.5.3. Substance testing regimes for ATCOs are in alignment with other aviation safety sensitive roles. Pilots have similar testing and substance requirements dictated by policies from airlines and the regulatory authorities.
2.5.4. MED 8.2.6 Substance Abuse in Air Traffic Control states that
IFATCA Policy is:
All appropriate safeguards and redress procedures should be established before the introduction of any mandatory drug-test scheme.
Mandatory drug tests, subject to the provisions above, are acceptable on initial recruitment of air traffic controllers to prevent any erosion of entry medical standards.
Mandatory drug tests, subject to the provisions above, of air traffic controllers in an ATC accident are acceptable in order to demonstrate positively their medical fitness at the time.
2.5.5. Testing methods may include analysis of saliva, breath, blood, urine and less common, sweat. Depending on the method used, traces of substances can be detected long after the psychoactive effects of the substance have subsided.
2.5.6. Self testing for the presence of substances may also be an option prior to the start of duty if an ATCO is unsure if they are ‘Under the Influence’ of either alcohol or psychoactive substances (either prescribed or illegal).
2.5.7. Several factors can influence how long a drug can be detected in a person’s system after consumption. These factors include the type of drug and its potency, the specific test used, the individual’s size and weight, their tolerance levels, and the presence of other drugs.
2.5.8. Current EASA requirements for Class 1 pilots as mentioned in MED.B.055 Mental Health (Annex IV Part-MED) state that (EASA, 2022):
- MED.B.055(b) Drugs and alcohol screening shall form part of the initial class 1 aero-medical examination.
- MED.B.055(c) Applicants with a mental or behavioural disorder due to use or misuse of alcohol or other psychoactive substances shall be assessed as unfit pending recovery and freedom from psychoactive substance use or misuse and subject to satisfactory psychiatric evaluation after successful treatment.
- AMC1 MED.B.055 (d) Psychoactive substance testing
- Drug tests should screen for opioids, cannabinoids, amphetamines, cocaine, hallucinogens and sedative hypnotics. Following a risk assessment performed by the competent authority on the target population, screening tests may include additional drugs.
- For renewal/revalidation, random psychoactive substance screening tests may be performed.[…]
- In the case of a positive psychoactive substance screening result, confirmation should be required in accordance with national standards and procedures for psychoactive substance testing.
- In case of a positive confirmation test, a psychiatric evaluation should be undertaken before a fit assessment may be considered by the medical assessor of the licensing authority.
- GM2 MED.B.055 (a) Drugs and alcohol screening tests used should:
- provide information regarding medium-term consumption
- be accepted on a national level by the competent authority based on the availability and suitability for the scope mentioned in point (a) (1) above.
2.6. Education and Consequences
2.6.1. Policies regarding positive test results must be clearly communicated and incorporated into education programmes. Response actions and consequences should be well-defined to ensure transparency and consistency.
2.6.2. Consequences for a positive test may include:
— Temporary withdrawal of ATCO license
— Loss of medical certification
— Treatment and rehabilitation
— Conditional or unrestricted return to duty
— Suspension or termination of employment
2.6.3. Adherence to ANSP drugs and alcohol management policies and regulations are likely an ATCO’s condition of employment. Policies should define the permitted level of concentration allowable for each class of drug or compound. Baseline thresholds or maximum allowable concentrations of a drug for test results need to be defined. These levels allow for accuracy and fairness and ensure that only a meaningful amount of the substance triggers a positive result and not just for incidental exposure. A positive test result exceeding this permitted level, even if the individual is not impaired, constitutes a breach of policy and a condition of employment.
2.7. Prescribed Medications
2.7.1. Another area of concern is the misuse of controlled substances, also referred to as pharmaceuticals, prescribed or over the counter medications. While these substances may be intended to treat everyday ailments, some can impair performance or result in a positive drug test—placing the individual in a compromising position. General practitioners may not be fully aware of the implications of prescribing a medication that affects the fitness for duty of an ATCO or that may trigger a positive test result.
2.7.2. For this reason, consultation with a certified aviation medical practitioner, who understands the operational and regulatory limitations for licence holders, should be the preferred point of contact.
2.7.3. If a medication is known to be required and does not impair fitness for duty but may result in a positive test, the ANSP or regulatory authority must be notified by the ATCO or their aviation medical practitioner. Transparency is essential to ensure regulatory compliance and to protect both the individual and operational integrity.
2.7.4. MED 8.2.1 Effects of Medicine Drugs and Alcohol states that
IFATCA Policy is:
Member Associations should approach their respective administrations to establish guidelines about the effects of the use of medicines, drugs, alcohol and other substances available in their country.
Where possible, individual substances, including trade names, should be identified and listed in order to give controllers guidance concerning the use of such substances and their compatibility with ATC work.
2.7.5. Prohibited pharmaceuticals for licence holders include but are not limited to sedatives, some pain medications, antihistamines, anticoagulants and certain antibiotics. Each regulatory authority should maintain a list of restricted or cautionary medications. ATCOs are personally responsible for ensuring that any medication used does not compromise their fitness for duty or breach regulatory standards. Advice and guidance from certified aviation medical practitioners should be sought if there are any concerns.
2.7.6. Conversely a licence holder that takes a prohibited pharmaceutical, through an informed choice and full knowledge their fitness for duty is compromised bears a responsibility to disclose this information to their ANSP proactively. This act of transparency should not be subject to punitive action as it is made in good faith with a commitment to maintaining operational safety standards.
2.7.7. The TPM has two main key policies relating to these matters which have been mentioned in part through this paper. MED 8.2.1 was amended last in 2001 and MED 8.2.6 “substance abuse” was created in 1991. Both need to be reviewed and edited as the terminology is outdated and some of the concepts no longer remain valid and need clarification. The term ‘abuse’ has a high association with negative judgements and alternatives need to be considered.
Conclusion
3.1. The use of psychoactive substances in aviation is governed by strict international standards to ensure safety and operational integrity.
3.2. As outlined in ICAO Annex 1, the expectations for licence holders are clear; they shall not engage in any problematic use of substances and shall not exercise the privileges of their licences and related ratings while under the influence of any psychoactive substance.
3.3. Most ANSPs have comprehensive drug and alcohol awareness programmes which aim to educate and inform staff about substance related risks, monitor compliance through testing regimens and provide medical assistance and rehabilitation treatment if deemed necessary. Failure to adhere to these regulations may result in serious consequences, including withdrawal of licence privileges, and in extreme cases, termination of employment.
3.4. To ensure fairness and consistency ANSPs should establish a clear testing and response process for managing non-negative results. These would include confirmatory testing, medical reviews, defined escalation and resolution paths and transparent communication of consequences and support options.
3.5. It is the ATCO’s responsibility to report fit for duty in order to carry out their duties with the utmost regard for safety, this includes not being impaired or under the influence of psychoactive substances. If an ATCO believes they are not fit for duty, they shall declare this to their ANSP without fear of punishment.
Recommendations
4.1. It is recommended that the following be amended in the TPM.
| IFATCA TPM (2025), MED 8.2.6 – Misuse of Substances Abuse in Air Traffic Control |
Proposal: An alcohol and other drug management and education programme All appropriate safeguards and redress procedures should be established before the introduction of any mandatory drug-test scheme. Mandatory drug tests, subject to the provisions above, are acceptable on initial recruitment of air traffic controllers to prevent any erosion of entry medical standards. Mandatory drug tests, subject to the provisions above, of air traffic controllers in an ATC accident are acceptable in order to demonstrate positively their medical fitness at the time. Any air traffic controller subjected to a drug test should receive a sealed identical sample in order to obtain an independent analysis paid by the employer. A programme of rehabilitation from substance abuse should be made available to an air traffic controller where a problem is recognised. This programme should be set up and conducted in consultation with the MA in order to maintain the confidence of the individual concerned without fear of a punitive response. |
4.2. Additionally, with respect to available resources and time, EVPP will coordinate with relevant committees and task forces to consider:
— conducting a policy review of the MED section of the TPM, and include it as part of the PLC working programme, and
— creating a briefing paper to release on IFATCA’s stance on use of cannabinoids (Inline with IFALPA’s); and/or
— creating guidance material for MAs regarding testing policies and education material; and/or
— developing an IFATCA training package related to the topic to be made available for MAs.
References
ATSB. Cannabis and its Effects on Pilot Performance and Flight Safety: A Review. Australian Transport Safety Bureau. 2004
CAA. The Problematic Use of Psychoactive Substances. Safety and Airspace Regulation Group Policy Statement, UK Civil Aviation Authority, 2021.
CAA. Policy on the Responsibilities of ATC Service Providers Regarding the Problematic Use of Psychoactive Substances. UK Civil Aviation Authority. 2021
Caplan, Y. H., and B. A. Goldberger. “Detection Windows of Drugs in Different Test Materials.” Journal of Analytical Toxicology, vol. 25, no. 5, 2001
CASA. Drug and Alcohol Testing: Employer Testing. Civil Aviation Safety Authority, Australia, 2026.
CCOHS. Impairment at Work – Policy and Recognition. Canadian Centre for Occupational Health and Safety, 2026.
EASA. MESAFE: Mental Health for Aviation Safety [EASA.2022.C07]. European Union Aviation Safety Agency, Annex III to ED Decision 2018/012/R.
Huestis, Marilyn A. “Human Cannabinoid Pharmacokinetics.” National Library of Medicine, PMC2689518, 2005 (Current as of 2026).
ICAO. Annex 1: Personnel Licensing. 14th edition, International Civil Aviation Organization, 2022
ICAO. Doc 8984: Manual of Civil Aviation Medicine. 3rd edition, 2012.
ICAO. Doc 9654: Manual on Prevention of Problematic Use of Substances in the Aviation Workplace. 1995.
IFALPA. Cannabinoids. Briefing Leaflet 25HUPBL04, International Federation of Air Line Pilots’ Associations, 2025.
Merriam-Webster. “Psychoactive Substance.” Merriam-Webster.com Dictionary, 2026.
Office of Drug Control (ODC). Controlled Substances. Australian Government Department of Health and Aged Care, 2026.
SEASR. Mind the gap. Why Gender Equity in Air Traffic Management Matters retrieved from https://www.sesarju.eu/news/mind-gap-why-gender-equality-air-traffic-management-matters 2024
Transport Canada. Cannabis Legalization and the 28-Day Abstinence Policy. Government of Canada, 2026.
Transport Canada. Civil Aviation Integrated Management System (IMS) Documents. Government of Canada, 2026.
WHO. Drugs (Psychoactive Substances). World Health Organization, 2026.

