
52ND ANNUAL CONFERENCE, Bali, Indonesia, 24-28 April 2013WP No. 162Electro Magnetic Hyper SensitivityPresented by PLC |
Summary
Following a case of an ATCO that was diagnosed with EHS – Electromagnetic Hyper Sensitivity, this working paper will describe what is known about this syndrome and provide information that can help ATCOs to cope with such symptoms and raise the awareness of EMF – Electro Magnetic Fields.
Introduction
1.1. As the technological innovation in ATM continues, there has been an unprecedented increase in the number and diversity of electromagnetic field (EMF) sources. The ATCO working environment is composed of a variety of electronic devices /electromagnetic field sources; these sources include video display units associated with computers or radar screens, radio instruments of various types, Wi-Fi, meters or even kilometers of electronic cables and wires.
1.2. While these devices have made our life/work richer, safer and easier, they have been accompanied by concerns about possible health risks due to their Electro Magnetic Field (EMF) emissions.
1.3. Most people do not react to or suffer any problems from this environment, while some individuals report mild symptoms and react by avoiding the fields as best as they can, others are so severely affected that they have to cease work and change their entire lifestyle.
1.4. Human beings are bioelectrical systems. Our hearts and brains are regulated by internal bioelectrical signals. Environmental exposure to artificial EMFs (electromagnetic fields) may interact with fundamental biological processes in the human body. In some cases, this may cause discomfort and disease.
1.5. The background level of EMF from electrical sources has risen exponentially, most recently by the popularity of wireless technologies such as cell phones, cordless phones, and WI-FI and WI-MAX networks (see note).
1.6. The sensitivity to EMF has been generally termed “electromagnetic hypersensitivity” or EHS (see note).
Note: Bio Initiative Report: A Rationale for a Biologically-based Public Exposure. Standard for Electromagnetic Fields (ELF and RF) Release Date: August 31, 2007.
This report has been written by 14 (fourteen) scientists, public health and public policy experts to document the scientific evidence on electromagnetic fields. Another dozen outside reviewers have looked at and refined the Report.
The purpose of this report is to assess scientific evidence on health impacts from electromagnetic radiation below current public exposure limits and evaluate what changes in these limits are warranted now to reduce possible public health risks in the future. Not everything is known yet about this subject; but what is clear is that the existing public safety standards limiting these radiation levels in nearly every country of the world look to be thousands of times too lenient. Changes are needed. New approaches are needed to educate decision-makers and the public about sources of exposure and to find alternatives that do not pose the same level of possible health risks, while there is still time to make changes.
Discussion
2.1. What is Electromagnetic Hyper Sensitivity (EHS)?
2.1.1. EHS is characterised by a variety of non-specific symptoms, which afflicted individuals attribute to exposure to EMF. The symptoms most commonly experienced include dermatological symptoms (redness, tingling, and burning sensations) as well as neurasthenic and vegetative symptoms (fatigue, tiredness, concentration difficulties, dizziness, nausea, heart palpitation, and digestive disturbances). The collection of symptoms is not part of any recognised syndrome.
2.1.2. EHS resembles multiple chemical sensitivities (MCS), a disorder associated with low-level environmental exposure to chemicals. Both EHS and MCS are characterised by a range of non-specific symptoms that lack apparent toxicological or physiological basis or independent verification. A more general term for sensitivity to environmental factors is Idiopathic Environmental Intolerance (IEI), which originated from a workshop convened by the International Programme on Chemical Safety (IPCS) of the world health organization (WHO) 1996 in Berlin. IEI is a descriptor without any implication of chemical etiology, immunological sensitivity or EMF susceptibility. IEI incorporates a number of disorders sharing similar non-specific medically unexplained symptoms that adversely affect people. However since the term EHS is in common usage it will continue to be used here.
2.1.3. Following a study conducted in 2005 (WHO, 2005), the World Health Organization (WHO) concluded that EHS has no clear diagnostic criteria and there is no scientific basis to link EHS symptoms to EMF exposure. EHS is characterised by a variety of non-specific symptoms that differ from individual to individual. The symptoms are certainly real and can vary widely in their severity. Whatever its cause, EHS can be a disabling problem for the affected individual. EHS has no clear diagnostic criteria and there is no scientific basis to link EHS symptoms to EMF exposure. Further, EHS is not a medical diagnosis, nor is it clear that it represents a single medical problem.
2.2. Prevalence
2.2.1. There is a very wide range of estimates of the prevalence of EHS in the general population. A survey of occupational medical centers estimated the prevalence of EHS to be between a few individuals per million in the population, to up to 5%. One of the reasons for this difference in estimates is the lack of defined diagnostic guidelines. Approximately 10% of reported cases of EHS were considered severe.
2.2.2. There is also considerable geographical variability in prevalence of EHS and in the reported symptoms. The reported incidence of EHS has been higher in Sweden, Germany, and Denmark for example, than in the United Kingdom, Austria, and France. Video Display Unite (VDU) -related symptoms were more prevalent in Scandinavian countries, and they were more commonly related to skin disorders than elsewhere in Europe. Symptoms similar to those reported by EHS individuals are common in the general population.
2.2.3. The prevalence among ATCOs is not known but we can assume that it, at least, match the general population.
2.3. Electromagnetic radiation
2.3.1. ‘To get an idea of the different forms of radiation hereafter the different types in the Electromagnetic Spectrum’ are explained. Radiation having a wide range of energies forms the electromagnetic spectrum; the spectrum has two major divisions:
- Non-ionizing radiation- Radiation that has enough energy to move atoms in a molecule around or cause them to vibrate, but not enough to remove electrons (ionizing), is referred to as “non-ionizing radiation.” Examples of this kind of radiation are sound waves, visible light, and microwaves;
- Ionizing radiation- Radiation that falls within the ionizing radiation” range has enough energy to remove tightly bound electrons from atoms, thus creating ions. This is the type of radiation that people usually think of as ‘radiation’. This radiation can be extremely dangerous but for specific use we also take advantage of its properties to generate electric power, to kill cancer cells, and in many manufacturing processes.
2.3.2. The relevant range to our working environment is the Non-ionizing radiation .The diagram below shows the radiation type, definition (non-ionizing, ionizing), source and effects. It can be seen that many of our daily electronic appliances at home or work are radiating non-ionizing radiation.
Types of Radiation in the Electromagnetic Spectrum
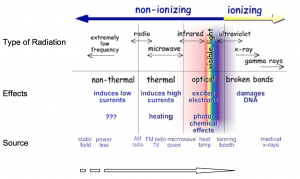
The energy of the radiation shown in the spectrum diagram above increases from left to right as the frequency rises.
2.4. Studies on EHS individuals
2.4.1. A number of studies have been conducted where EHS individuals were exposed to EMF similar to those that they attributed to the cause of their symptoms. The aim was to elicit symptoms under controlled laboratory conditions.
2.4.2. The majority of studies indicate that EHS individuals cannot detect EMF exposure any more accurately than non-EHS individuals. Well controlled and conducted double-blind studies have shown that symptoms were not correlated with EMF exposure.
2.4.3. It has been suggested that symptoms experienced by some EHS individuals might arise from environmental factors unrelated to EMF. Examples may include “flicker” from fluorescent lights, glare and other visual problems with VDUs, and poor ergonomic design of computer workstations. Other factors that may play a role include poor indoor air quality or stress in the workplace or living environment.
2.4.4. There are also some indications that these symptoms may be due to pre-existing psychiatric conditions as well as stress reactions as a result of worrying about EMF health effects, rather than the EMF exposure itself.
2.4.5 In January, 2010 Rubin et al published a follow up to their original review which included 15 experiments done since the last original review, bringing the totals up to 46 double-blind experiments and 1175 individuals with claimed hypersensitivity. The study confirmed the results of the original, claiming “no robust evidence could be found” to support the hypothesis that electromagnetic exposure causes EHS.
2.4.6 Electromagnetic hypersensitivity is not currently an accepted diagnosis. At present there are no accepted research criteria other than ‘self-reported symptoms’, and for clinicians there is no case definition or clinical practice guideline. There is no specific test that can identify sufferers, as symptoms other than skin disorders tend to be subjective or non-specific.
2.4.7 It is important firstly to exclude all other possible causes of the symptoms. Researchers and the WHO (World Health Organization) have stressed the need for a careful investigation. For some, complaints of electromagnetic hypersensitivity may mask organic or psychiatric illness and requires both a thorough medical evaluation to identify and treat any specific conditions that may be responsible for the symptoms and a psychological evaluation to identify alternative psychiatric/psychological conditions that may be responsible for or contribute to the symptoms.
2.4.8 A WHO factsheet also recommends an assessment of the workplace and home for factors that might contribute to the presented symptoms. These could include indoor air pollution, excessive noise, poor lighting (flickering light) or ergonomic factors. They also point out that some studies suggest that certain physiological responses of electromagnetic hypersensitivity individuals tend to be outside the normal range. In particular, hyper reactivity in the central nervous system and imbalance in the autonomic nervous system need to be followed up in clinical investigations and the results for the individuals taken as input for possible treatment.
2.5 EMF Radiation Standards
2.5.1 What is the approved/recommended radiation standard? How can we be sure that the environment we live/work is safe?
2.5.2 What is the basis on which these standards were made? And why it is important to us to know them?
2.5.3 If the use of mobile phone is taken as an example, the data about the amount of radiation omission is a factor that is being emphasised in the technical and commercial data sheets. A cell phone’s SAR, or its Specific Absorption Rate, is a measure of the amount of radio frequency (RF) energy absorbed by the body when using the handset. All cell phones emit RF energy and the SAR varies by handset model, for a phone to receive certification and be sold in the United States and Canada, its maximum SAR level must be 1.6 watts per kilogram, while in Europe the level is capped at 2 watts per kilogram.
2.5.4 The list below is taken from the website CNET, for the full lists please refer; it shows the levels of SAR for popular models, this list emphasize the growing awareness of the public and the manufacturers to the radiation level data.
Lowest SAR mobile phone
Samsung Galaxy Note 0.19
Samsung Galaxy S II 0.30
Kyocera DuraXT 0.328
Highest SAR mobile phone
BlackBerry Curve 9310 1.58
Nokia Astound 1.53
Motorola Razer HD 1.56
2.5.5 ICNIRP Occupational threshold (see note), 2500 microwatts/cm2-
CNIRP is the International Commission on Non-Ionizing Radiation Protection. This occupational threshold is based on the radiation level that causes body heat raise in 1c°
2.5.6 ICNIRP General public threshold (see note), 500 microwatts/cm2
This threshold is reduced by 5 times from the occupational threshold due to the fact that the general public is not aware of the risk and does not take any precautions.
Example of environmental threshold:
Israel: 50 microwatts/cm2
Italy: 2.5-10 microwatts/cm2
Switzerland: 2.5-10 microwatts/cm2
Note: CNIRP is the International Commission on Non-Ionizing Radiation Protection. It is a body of independent scientific experts consisting of a main Commission of 14 members, 4 Scientific Standing Committees covering Epidemiology, Biology, Dosimetry and Optical Radiation and a number of consulting experts. This expertise is brought to bear on addressing the important issues of possible adverse effects on human health of exposure to non-ionizing radiation. ICNIRP’s principal aim is to disseminate information and advice on the potential health hazards of exposure to non-ionizing radiation to everyone with an interest in the subject.
2.5.7 The European parliamentary assembly, May 2011, stated;
“reconsider the scientific basis for the present electromagnetic fields exposure standards set by the International Commission on Non-Ionizing Radiation Protection, which have serious limitations and apply “as low as reasonably achievable” (ALARA) principles, covering both thermal effects and the athermancy or biological effects of electromagnetic emissions or radiation” “pay particular attention to “electro sensitive” persons suffering from a syndrome of intolerance to electromagnetic fields and introduce special measures to protect them, including the creation of wave-free areas not covered by the wireless network;”
2.5.8 The Lichtenstein parliament adopts the recommended threshold set by the BIOINITIATIVE report and has decided to reduce the public exposure to radiation as low as 0.1 microwatts/cm2 till the year 2013.
2.5.9 Example from ATM:
2.5.9.1 The standard used at Swanwick UK (NATS) is BS EN55014-1, which covers domestic and office equipment. This has the lowest levels for the generation of EM radiation, but also has lower immunity. The standard is related to the European standard, such that they generally take the CE mark as proof of compatibility to this standard. In the case of special build equipment, it is sent to an external test house to ensure compliance. Measurements of the levels of RF radiation are not generally undertaken, unless they are specifically asked for, but, measurements have been taken on site to assess the levels of EM radiation within various areas of the building, and how much escapes. Measurements have also been taken to assess the susceptibility of the building to external EM radiation. All of these measurements have been undertaken by specialist external contractors. Due to the way power is transmitted around the site, monitoring the performance of new equipment with regard to power line harmonic generation (power factor), which is also covered by the CE mark, but looks for a very high standard, and are checked for compliance.
2.5.9.2 The standard applied in Israel is according to the ICNIRP recommendation, The Israeli airport authority has a clear regulation that every facility must be checked once a year by an independent expert company according to the standards of the Israeli ministry of environmental protection. The report is submitted to management and published to the relevant units. The radiation levels from the last report showed a much lower radiation levels than the maximum approved.
2.5.10 Today public exposure limits for telecommunications are based on the presumption that heating of tissue (for RF) or induced electric currents in the body (for extremely low frequency electromagnetic fields ELF) are the only concerns when living organisms are exposed to RF. These exposures can create tissue heating that is well known to be harmful in even very short-term doses. Bio effects and some adverse health effects occur at far lower levels of RF and ELF exposure where no heating (or induced currents) occurs at all; some effects are shown to occur at several hundred thousand times below the existing public safety limits where heating is an impossibility. Effects occur at non-thermal or low-intensity exposure levels thousands of times below the levels that federal agencies say should keep the public safe. For example, very low-level ELF and RF exposures can cause cells to produce stress proteins, meaning that the cell recognizes ELF and RF exposures as harmful. This is another important way in which scientists have documented that ELF and RF exposures can be harmful, and it happens at levels far below the existing public safety standards. Many new devices operating with wireless technologies are exempt from any regulatory standards. The existing standards have been proven to be inadequate to control against harm from low-intensity, chronic exposures, based on any reasonable, independent assessment of the scientific literature. It means that an entirely new basis (a biological basis) for new exposure standards is needed. New standards need to take into account what we have learned about the effects of ELF and RF, all non-ionizing electromagnetic radiation, to design new limits based on biologically demonstrated effects that are important to proper biological function in living organisms.
The current situation
3.1 EHS has no clear diagnostic criteria and there is no scientific basis to link EHS symptoms to EMF exposure. Further, EHS is not a medical diagnosis, nor is it clear that it represents a single medical problem.
Physicians: Treatment of affected individuals should focus on the health symptoms and the clinical picture, and not on the person’s perceived need for reducing or eliminating EMF in the workplace or home. This requires:
- A medical evaluation to identify and treat any specific conditions that may be responsible for the symptoms,
- A psychological evaluation to identify alternative psychiatric/ psychological conditions that may be responsible for the symptoms,
- An assessment of the workplace and home for factors that might contribute to the presented symptoms, reduction of stress and other improvements in the work situation might be appropriate.
3.1.1 For EHS individuals with long lasting symptoms and severe handicaps, therapy should be directed principally at reducing symptoms and functional handicaps. This should be done in close co-operation with a qualified medical specialist (to address the medical and psychological aspects of the symptoms) and a hygienist (to identify and, if necessary, control factors in the environment that are known to have adverse health effects of relevance to the patient).
Treatment should aim to establish an effective physician-patient relationship, help develop strategies for coping with the situation and encourage patients to return to work and lead a normal social life.
EHS individuals: Apart from treatment by professionals, self help groups can be a valuable resource for the EHS individual.
3.2 Nordic approach
3.2.1 This is an extract from the Nordic co-operative project called “The Nordic Adaptation of Classification of Occupationally Related Disorders (diseases and symptoms) to ICD-10”, financed by the Nordic Council of Ministers (Nordisk Ministerråd) and completed 1996 to 2000.
3.2.2 The aim of the project was to provide a “Nordic list of occupational disorders” with advice on how to code them in accordance with the WHO International Statistical Classification of Diseases and Related Health Problems (ICD) version 10.
3.2.3 Disorders caused by occupational exposure and for some groups of not well- specified conditions, which in the Nordic countries are claimed, but not yet proven, to be caused by occupational exposures.
R68.- Other general symptoms and signs
R68.8 Other specified general symptoms and signs
(Suggested/recommended for multisymptomatic “idiopathic/environmental intolerance” (IEI), including “multiple chemical sensitivity” (MCS); “electromagnetic intolerance” (“el-allergy”) etc. if the patient has not one major symptom which should preferably be coded)
3.3 Spanish case
3.3.1 In September 2011 Social Court 24 of Madrid, declared a university professor, who suffered chronicle fatigue syndrome and electromagnetic and environmental hyper-sensitivity, as permanently incapacitated.
3.3.2 The court verdict is unique on this aspect and it will set a precedent for future pathologies related to the hyper-sensitivity to these specific types of waves. This verdict was dictated last May 23 and granted to the professor 100% of his basic salary, which was 1640, 80 Euros.
3.3.3 The social security incapacity valuation team (E.V.I.), recognised as a valid clinic diagnostic of the patient: chronicle fatigue syndrome, celiac disease, fibromyalgia and the electromagnetic and environmental hyper-sensitivity syndrome.
3.3.4 The social court of Madrid is again questioning the criteria to concede this grade (of incapacity, referring to the 100%) of the Province Directorate of the National Institute (of social security), and it recognises the rights of the petitioner by affirming (the social court in the verdict) that the petitioner presents enormous problems to accomplish her tasks “with an adequate level of professionalism and performance”.
Conclusions
4.1 EHS is characterised by a variety of non-specific symptoms that differ from individual to individual. The symptoms are certainly real and can vary widely in their severity. Whatever its cause, EHS can be a disabling problem for the affected individual.
4.2 EHS has no clear diagnostic criteria and there is no scientific basis to link EHS symptoms to EMF exposure. Further, EHS is not a medical diagnosis, nor is it clear that it represents a single medical problem
4.3 Except Sweden and one court case in Spain, EHS is not recognised as an occupational illness.
4.4 There is no specific or clear radiation standard /threshold for ATM facilities nor any regulated monitoring requirement.
4.5 MAs should approach their ANSP to verify any appropriate standards. Periodic radiation level checks should be conducted in ATC operation rooms and control towers. The radiation level in ATC operation rooms and control towers shall match the lowest appropriate radiation standard in order to mitigate the risk of radiation.
Recommendations
This paper is accepted as information.
References
Bio Initiative Report: A Rationale for a Biologically-based Public Exposure. Standard for Electromagnetic Fields (ELF and RF) Release Date: August 31, 2007.
ICNIRP Guidelines: GUIDELINES FOR LIMITING EXPOSURE TO TIME-VARYING ELECTRIC, MAGNETIC, AND ELECTROMAGNETIC FIELDS (UP TO 300 GHz) International Commission on Non-Ionizing Radiation Protection, 1998.
DR. Steven Gelberg, Ministry of Environment, Israel.
Italian Regulation DECREE OF THE PRESIDENT OF THE COUNCIL OF MINISTERS 8 JULY 2003 Establishment of exposure limits, attention values, and […].
Ordinance relating to Protection from Non-Ionising Radiation (ONIR) of 23 December 1999 (as of 1 February 2000).
The Nordic Adaptation of Classification of Occupationally. Related Disorders (Diseases and Symptoms) to ICD-10
(ICD-10: International Statistical Classification of Diseases and Related Health Problems) Editors: Finn Levy, Department of Occupational Medicine, Center for Preventive Medicine (1K), Ullevaal University Hospital, Oslo; Axel Wannag, Directorate of Labour Inspection, Oslo, 2000.
Cardiovascular risk in operators under radiofrequency electromagnetic radiation. Vangelova K, Deyanov C, Israel Int J Hyg Environ Health. 209(2):133-138, 2006.
Hillert, L; N Berglind, BB Arnetz, T Bellander (February 2002). “Prevalence of self-reported hypersensitivity to electric or magnetic fields in a population-based questionnaire survey”.Scand J Work Environ Health 28 (1): 33–41. PMID 11871850.
Levallois, P; R Neutra, G Lee, L Hristova (August 2002).”Study of self-reported hypersensitivity to electromagnetic fields in California”. Environ Health Perspect 110 (Suppl 4): 619–23.
Eltiti S, Wallace D, Zougkou K, et al. (February 2007). “Development and evaluation of the electromagnetic hypersensitivity questionnaire”. Bioelectromagnetics 28 (2): 137–51.
Rubin, James; J Das Munshi J, Simon Wessely (March–April 2005). “Electromagnetic hypersensitivity: a systematic review of provocation studies”. Psychosomatic Medicine 67 (2): 224–32.
Röösli M (June 2008). “Radiofrequency electromagnetic field exposure and non-specific symptoms of ill health: a systematic review”. Environ. Res. 107 (2): 277–87.
Rubin, James; Rosa Nieto-Hernandez, Simon Wessely (January 2010). “Idiopathic Environmental Intolerance Attributed to Electromagnetic Fields”. Bioelectromagnetics 31 (1): 1-11.
The International Commission on Non-Ionizing Radiation Protection (CNIRP). https://www.icnirp.de
Electromagnetic compatibility. Requirements for household appliances, electric tools and similar apparatus. Emission British-Adopted European Standard / 31-Jan-2007 / 86 pages. https://www.thetechstandard.com/BS-EN-55014-1-2006-A1-2009
The European Low Voltage Directive: https://ec.europa.eu/enterprise/sectors/electrical/lvd/
https://reviews.cnet.com/cell-phone-radiation-levels/
“Electromagnetic fields and public health: Electromagnetic Hypersensitivity”. WHO Factsheet 296. World Health Organisation (WHO). December 2005. Retrieved 2012-10-24.
Hillert, L; N Berglind, BB Arnetz, T Bellander (February 2002). “Prevalence of self- reported hypersensitivity to electric or magnetic fields in a population-based questionnaire survey”.Scand J Work Environ Health 28 (1): 33–41. PMID 11871850.
Levallois, P; R Neutra, G Lee, L Hristova (August 2002). “Study of self-reported hypersensitivity to electromagnetic fields in California”. Environ Health Perspect 110 (Suppl 4): 619– 23.doi:10.1289/ehp.02110s4619. PMC 1241215. PMID 12194896.
Schreier N, Huss A, Röösli M (2006). “The prevalence of symptoms attributed to electromagnetic field exposure: a cross-sectional representative survey in Switzerland”. Soz Praventivmed 51 (4): 202–9. doi:10.1007/s00038-006-5061-2. PMID 17193782.

